
If I live to be 100 years old, I don’t think I’ll EVER understand how my brain processes information. I definitely have trouble staying in my lane when it comes to how I visualize and analyze things. Here’s a perfect example:
My wife and I were on a trip, and we stopped to eat at a medium-price, family restaurant. This particular place has lots of entrees in the $10-$15 range, all very tasty, with healthy options, too. I had walked by a salad bar on my way in and noticed that it looked full and well-kept.
In fact, for $3 you can add unlimited salad bar to any order, according to our server, Tess. My wife and I both added the option. When we got to the bar, this is what we saw:
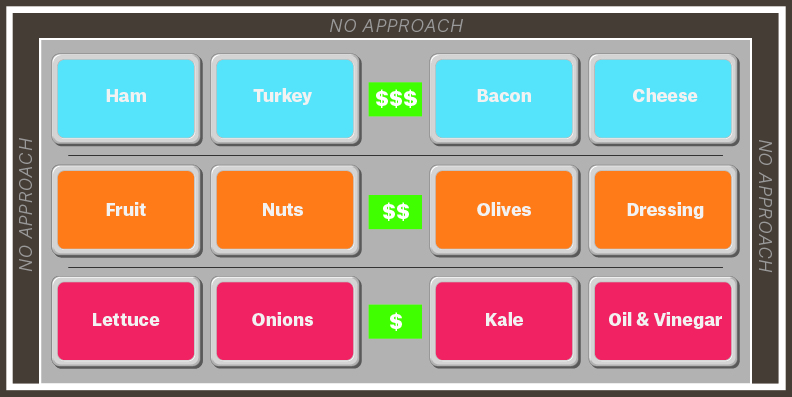
Almost immediately, my wife had problems. She’s about 5’5” and her arms were not long enough to make it past the LARGE sneeze guard and the first two rows of salad greens, olives and dressings to get to the third row. Being taller and with longer arms, I helped her out by reaching some of the protein choices in the back, like the bacon, turkey and cheese.
To me, it seemed this ONE-SIDED SALAD BAR was designed to force you to access it from the side with the cheapest ingredients. Easy to see this design allowed the restaurants to keep costs to a minimum by making the more expensive, protein-laden choices much more difficult to access. Entirely rational, if a little sneaky.
As we carried our plates back to the table, I could NOT get that image out of my mind. And then it hit me… that SINGLE-SIDED SALAD BAR was a really good analogy for how health systems like the provincial programs in Canada or the National Health System in the United Kingdom control costs as well. It also applies to Medicaid here in the U.S., but for entirely different reasons.
Wherein Cheese = Neurosurgery
Check out this image:
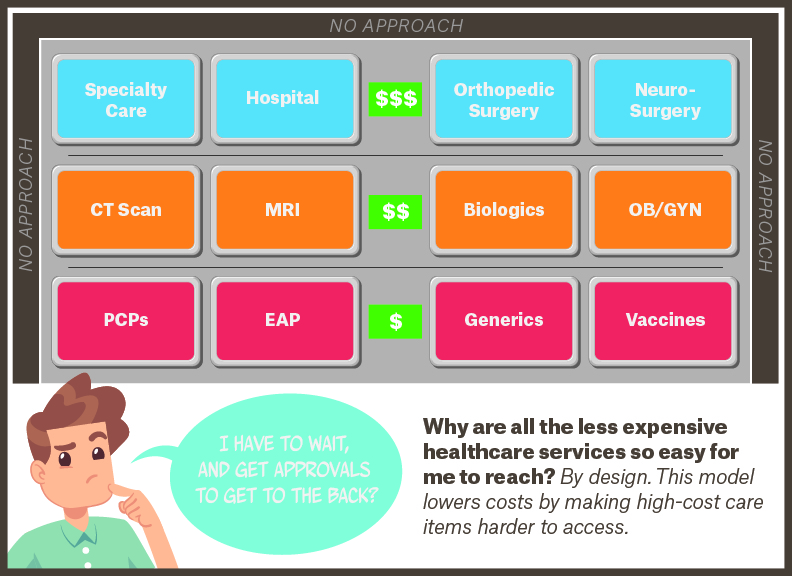
The Single-Sided Salad Bar Rationing Model Applied to Universal Healthcare (Canada, U.K. NHS)
“Rational” healthcare systems, like those found in other developed countries, tend to establish gatekeepers over all care, but some care that is inexpensive and good for many people is put within easy reach.
In this version above, you can see Primary Care Provider (PCP) visits, Employee Assistance Program (EAP)-type mental health visits, generic drugs and vaccines are very easy to access. Advanced imaging (like MRIs and CT Scans), specialty care or biologic drugs are much tougher to reach, and the PCPs are the gatekeepers of the entire system.
Since care is rationed by strict cost control, wait times for many procedures can get pretty lengthy, much longer than most people would tolerate here in the U.S (See my Straight Talk Article “Baseball, Cataracts, and Single Payer”). But there is only one way in, so people who aren’t satisfied with the wait have no other options.
Care in the U.K. is free once you get it, but it is funded by an embedded 20% sales tax on every transaction, even wholesale. To get that care, you have to be registered with a PCP and give him/her control over all your healthcare decisions, including referrals up to specialty care. PCPs are employed by the government (health districts) and have obligations to both their patients and their employer as gatekeepers of the entire healthcare system.
Is Medicaid a Single-Sided Salad Bar?
So if this is how it looks in the U.K., what about here in the U.S.?
The first system I thought about was Medicaid. Now that more than 73 million people on our government-funded single payer free healthcare system, it’s important that we understand how it differs from both the European/Canadian models and our other U.S. systems like Medicare.
Here’s what Medicaid looks like in comparison:
The Single-Sided Salad Bar Rationing Model Applied to Medicaid
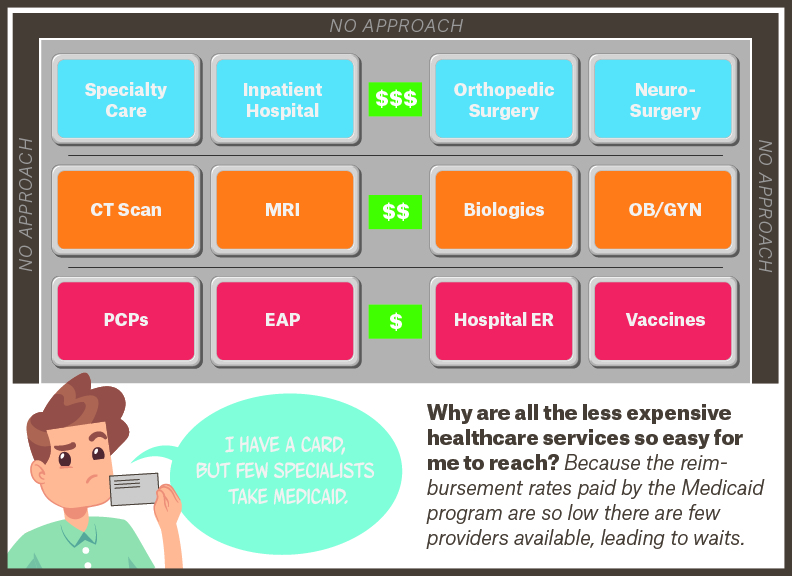
Notice that here in the U.S., our Medicaid program is a SINGLE-SIDED SALAD BAR just like in the U.K. or Canada, but for very different reasons. Instead of rationing based on very tight treatment protocols via gatekeeper primary care, the rationing here is unintentional. It is a by-product of the fact that Medicaid’s reimbursement levels to medical providers are so low. In fact, they are 30-40% below the WHOLESALE cost of providing treatment.
This means as a medical practice fills up with Medicaid patients, its financials slowly deteriorate until it begins to ration or limit the slots available for Medicaid patients. It’s already happening at smaller hospitals and at least one not-for-profit nursing home.
Patients on Medicaid can go to a PCP or a Federally Qualified Health Center (FQHC) and get primary care, even an appointment with a specialist. But that specialist appointment may be for six months from now, or longer, because so few specialists can operate on what Medicaid pays.
So, in the U.S., we have rationing by underpayment, which means longer wait times for the patients.
UNLIKE the U.K., or Canada, you’ll notice I put the “Hospital ER” box in the easy-to-access, first row of the Medicaid model. That’s by design. In the U.S., Medicaid patients are MUCH more likely to use the ER or urgent care center than they are to visit a doctor’s office. It turns out that the MOST expensive care a Medicaid patient can get is the easiest to access.
The U.S. Is a Double-Sided Salad Bar
Now, let’s take a look at the part of our system that is unique in the world and drives a significant portion of the costs that separate us in terms of spending. Here in the U.S., the 200+ million people on Medicare or private insurance are enjoying the DOUBLE-SIDED SALAD BAR model. Looks like this:
The Double-Sided Salad Bar Model Applied to Medicare, Private Coverage
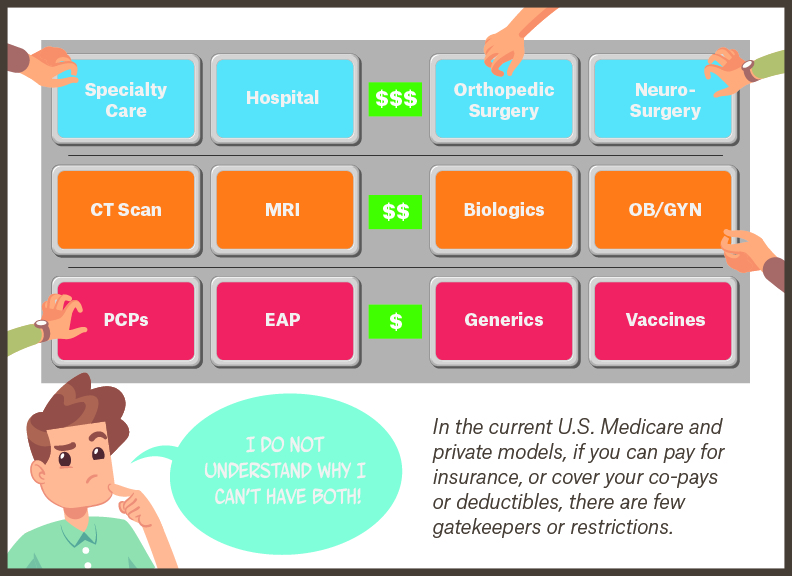
Notice that these happy people can access the healthcare salad bar in a variety of ways. In most cases, there are no requirements that they go through a gatekeeper; easy access and total control of their healthcare comes from the DOUBLE-SIDED SALAD BAR. If I have Medicare or private insurance, I can access whatever care I want, pretty much whenever I want. There are tons of resources in specialty care, surgical care, labs, imaging centers, pharmacies and the like, just waiting to fulfill my needs immediately.
I recently experienced this myself when my eye doctor told me I would benefit from cataract surgery. I wrote about that extensively here. In most countries, this is considered a luxury, non-essential surgery and eight or 10 months of wait time is not out of the ordinary. Plus, your PCP has to approve your specialist appointment ahead of time, or you don’t get to see the eye doctor at all.
Here in the U.S., I went straight to an ophthalmologist who scheduled my first surgery for five days later, then APOLOGIZED FOR THE WAIT BECAUSE THEY WERE BACKED UP! That’s the power of the double-sided salad bar of healthcare. Of course, all that choice comes with two big problems: high costs and complexity. And the73 million Medicaid patients pay $0 for care but don’t have access to a rich slew of choices and prompt service.
Are We Ready to Give Up the Double-Sided Salad Bar?
Now we are at the crux of this discussion. Much is being made of creating new healthcare insurance choices for Americans called “single payer,” “Medicare for all” or some other name for a government-run and managed system. So, I ask you this:
Are the 200 million people in the U.S. (including you) with access to the double-sided salad bar ready to surrender that access? Are you ready to wait? Are you ready to surrender even more authority to a large government agency and give up your own authority?
And the biggest question of all: How do you respond when a politician promises you can keep your double-sided salad bar but only pay the price of access to the single-sided salad bar?
Because that’s what is happening: a siren song that “Your government can do a better job, keep you happy, save you money and ask nothing of you.”
You know what they say: if it sounds too good to be true, it probably is.
Consider that two-thirds of the 55 million people on government-run Medicare buy private insurance to fill in the gaps OR a private policy that completely replaces Medicare. Coincidentally, the privately insured Medicare patients are the ones who report they are MOST SATISFIED with Medicare!
The federal agency that manages Medicare/Medicaid has only 4,000 employees to manage healthcare for 130 million people. How are they doing? The Government Accountability Office says they lose $60 billion each year due to fraud, waste and abuse; that’s around 10% of the U.S. government’s total healthcare budget. What happens if we give them MORE money and responsibility?
And finally, it’s worth noting that the federal agency that manages Medicare hasn’t processed a claim, enrolled anyone or done any of their own auditing since 1965 when they were formed. They outsource ALL of these functions to existing private insurance companies.
Which salad bar do you want to use?
Just food for thought! And the Straight Talk on Single-Payer/Medicare-for-all.



We already have long wait times – https://www.forbes.com/sites/brucejapsen/2017/03/19/doctor-wait-times-soar-amid-trumpcare-debate/#44b683542e74
We ration care by how much money you have in your pocket where other nations ration care by NEED.
Medicare for All has a 70% approval rating.
Medicare is not Medicaid.
Medicare has a 77% approval rating.
Medicare is more efficient than private insurance – https://www.healthaffairs.org/do/10.1377/hblog20110920.013390/full/
The United States paid 3.5 TRILLION for healthcare last year. Medicare for All is estimated to cost 1.4 Trillion. Last time I checked, 1.4 trillion is a net savings of 2.1 trillion.
35,000-45,000 people die annually due to lack of healthcare.
23% of Americans are underinsured.
44 million Americans are UNINSURED.
Medical bankruptcy is a leading cause of bankruptcy in the US.
We pay twice as much as other nations and receive WORSE outcomes.
The United States healthcare system ranks 37th IN THE WORLD behind nations who all have a single payer system – https://www.who.int/healthinfo/paper30.pdf
Seems like you don’t know your facts.
David! Thanks so much for all the wonderful links to the news reports and facts that you have quoted!
Although I do appreciate the passion, and breadth of your response, you will note that I am simply pointing out two irrefutable facts about any US move to a Single Payer/Medicare for all system. Facts that I worry will not be conveyed to voters before they are asked to make such a huge choice. Our members and all of the 170m plus people who have private insurance today deserve to know these outcomes are certain.
1. A government/funded, single payer system will have significantly longer wait times than any one of the 200m+ Americans who are on private insurance or private Medicare experience today. Interesting that you quoted the Japsen article above (I am familiar with Bruce’s work and read the article when he published it originally), which actually included Medicaid (a Single payer system) AND Medicare patients in the mix to determine that wait times are going up (to a level still nowhere near the wait times quoted in the UK or Canada). We can already see this today where care is rationed in Medicaid by lower reimbursements. You mentioned the high satisfaction rates with Medicare, which is entirely accurate. What you failed to mention was that almost 70% of Medicare members are on completely private versions of Medicare, run and managed by insurance companies, or are purchasing out of their own pockets, supplemental private insurance for hundreds of dollars per month because of the significant gaps in government-issue Medicare. In fact, if you took Medicare Parts A, B, and D, and created a health plan from them, it would NOT QUALIFY FOR SALE on http://www.healthcare.gov because of the large financial gaps in the program. This is why the most satisfied Medicare recipients are the ones with the PRIVATE versions of medicare. https://www.bettermedicarealliance.org/newsroom/press-releases/seniors-highly-satisfied-medicare-advantage
It’s also worth remembering, although I didn’t make a big deal out of it in the article, that the countries with much lower costs than the US all use gatekeeper primary care, meaning your specialist or surgical access is controlled by your PCP. This plus lower physician/surgeon salaries and lower drug costs are the primary way they are able to deliver care at lower costs. We tried this in the 90’s and medical costs actually went negative for a few years, but that loss of control was fought at every level of society until HMO’s vanished from the landscape for quite a number of years. The media was especially vocal against gatekeeper primary care (and still is).
2. Taxes will go up. No matter how much “efficiency” you attribute to Medicare, or Medicaid, you cannot absorb 170 million new patients without transitioning a lot of insurance premiums, deductibles, and co-payments into tax revenue, moving them from a category the average person can choose to pay, into a category he cannot choose to avoid. In addition, the research you quoted on straight government-issue Medicare being more efficient than private insurance was hotly contested, both by the CBO and the GAO, who continue to attribute over $50B a year in lost money (around 10% of their allocation) to structural weaknesses in Medicare/Medicaid. https://www.gao.gov/products/GAO-18-660T
Let’s also remember that CMMS, in its current form, only has about 4,000 employees to run a health care financing program for around 120 million people. This means that they outsource nearly everything. Private insurance companies pay the claims, process the enrollments, handle the appeals, and even enforce plan designs on behalf of CMMS. Even straight “government-issue” medicare has a significant private insurance company back office presence. Ramping up the government to handle all these functions internally is almost never figured into the cost estimates of “savings” in Single Payer/Medicare for all.
Check Kaiser’s research on Single Payer/Medicare for all and you will see that your “Medicare For All” 70% approval numbers drop into the low 20% range when the same folks surveyed are exposed to the truth of higher taxes or delays in care. https://www.kff.org/slideshow/public-opinion-on-single-payer-national-health-plans-and-expanding-access-to-medicare-coverage/
I’m not interesting in pillorying any particular healthcare payment model, but what we are dealing with here is far too important to ask folks to give up what they have without complete, transparent knowledge of what they are moving into. Higher taxes and delays in care are inevitable and our members deserve to know this.
That’s the point of this article. To make sure regular folks know taxes will go up, and wait times will go up as well. Period.
Thanks again for your thorough and well-thought out response!….mrb
So how are we addressing:
35,000-45,000 people die annually due to lack of healthcare
23% of Americans are underinsured
44 million Americans are UNINSURED
CJ!
Thanks so much for your comments on this article! Your points are important and need to be fleshed out and discussed.
It’s a clear tragedy that so many people die annually due to a lack of healthcare. We all need to do more to reach down into disadvantaged communities and help them understand what healthcare financial support is available and more importantly, how to access that care.
For example, Medicaid in Louisiana has expanded and over 500,000 people have signed up since the Summer of 2016 in our state. This has reduced the uninsured deaths in Louisiana to nearly zero. But many of these folks still use the Emergency Room as their primary point of care, meaning their chronic conditions like diabetes, high blood pressure, kidney and cardiac diseases are not being managed. By the time things get bad enough for them to go to the ER, often it’s too late to get them back on their feet. There are a variety of reasons why new Medicaid patients don’t go to the doctor regularly as they should. It might be a lack of knowledge, or transportation, or even trust. This is made worse by the fact that Medicaid pays docs so poorly that many cannot afford to see Medicaid patients and don’t take new ones. Some of this can be fixed by technology, but much of it is cultural and will take some time.
AT BCBSLA, transparency and education are the key strategies we are using, along with our predictive modeling and data collection to try and head off these problems before they occur. It’s always best if we can get folks to have an ongoing relationship with a PCP, and to make their appointments, even if it means we provide transportation for them at some point. That relationship is key to living a longer and healthier life for our citizens.
Almost all the Americans who fall into the “under-insured” category have deductibles that are higher than the money they have in the bank or live in a state that has not expanded Medicaid. The ACA has forced much higher deductibles onto our Individually Insured populations and Small Group populations than we would have liked, since the Feds are in control of the benefit designs and value our plans are allowed to provide. This is a much bigger problem in the 15 states that have not adopted the Medicaid expansion than it is here in Louisiana. Allowing low income folks to access free healthcare like we do here is the key to eradicating under-insurance.
The best data I have shows that the majority of the 44m people without insurance in the United States are those that are low income and live in states without Medicaid expansions. In addition, the undocumented immigrant population was shut out completely from ACA benefits in the original bill, and remain ineligible for low cost or free health insurance. They are included in the 44m number you quoted above. That may be as many as 13-15m folks without low cost or free access to care that currently live in the US because of their status.
I’m glad you pointed out these things. We have an obligation to work on them and fix them. It would be short-sighted, and wrong, in my opinion however, to force 200 million people (Medicare plus privately insured) out of the coverage they already have (and approve of with survey numbers in the high 70% range) just to cover the 44 million you mentioned.
Keep those thoughts coming! We need to keep having this debate until the problems are solved!
thanks..mrb